

Many women think that after they've had a breast augmentation, their journey is over. For some, yes, it will be. For others, however, their odyssey will pick back up in the years to come.
So before you have a breast augmentation, understand that no matter the skill of your breast implant surgeon, complications (or personal reasons) can arise, leading you back to the operating table and tossing more money at your initial investment.
Common problems that could lead to breast implant revision
Breast augmentation is often assumed to be simple in nature and execution when, in reality, it is quite complex. This means that problems can and do occur. And when they do, breast revision surgery is the solution to removing your dissatisfaction and getting you loving your breasts.
The problems that lead to breast implant revision may be on account of your surgeon, the implant itself, or your anatomy.
Implant malposition
Breast implants that ride high, are too close together, fall too low, or spill out toward the armpits, are displaced and not properly positioned behind the breast. As a result, the breasts look odd and distorted.
1. Implant asymmetry
Your breasts are sisters, not twins; meaning one might sit higher or drift further outward or inward than the other. If during the planning process your breast augmentation does not include methods to try to stabilize symmetry by inserting different implant sizes or shapes or by adjusting the inframammary fold, your breasts will be asymmetrical even after surgery.
Still, symmetry may not be fully achieved despite your surgeon's best efforts. One implant—due to tension on the breast tissue—may refuse to settle while the other falls into position. Or, gravity, aging, and other natural factors may come into play, leaving the breasts malpositioned over time.
Repair: If your breast implants are uneven due to tension on the breast tissue, breast revision surgery can be used to release the tissue so that it is resting at the same height as the other. If asymmetry is on account of natural factors, surgical scaffolds may be needed to lift the lower-riding breast implant higher on the breast mound or a breast lift (mastopexy) procedure could be used to reshape and lift both breasts.
2. Bottoming out (low malposition)
When your skin and underlying breast tissue are too thin or lax to support the weight of your implant, or if your breast pocket was over-dissected near the breast crease, the implant can slip from the pocket, causing it to descend toward the inframammary fold and push the nipple higher on the breast mound, so that it points upwards. The implants, as a result, become asymmetrical.
Repair: In the case of bottoming out, your surgeon can reinforce the breast pocket with durable, permanent sutures or surgical mesh, both of which are designed to act as a scaffold and hoist the lower-riding implant up. Mastopexy (breast lift) is also an option, as is replacing the original breast implants with smaller ones.
3. Symmastia (uniboob)
Your anatomy dictates the implant sizes your breasts are able to comfortably hold. When you enlist your plastic surgeon to go beyond your anatomy and force it to fit or support large breast implants, he must over-dissect your breast pocket. Dissecting passed the sternum can cause the breasts to touch in the middle and the skin to lift off the sternum. You may have desired more cleavage and bigger breasts, but what you end up with is what appears to be a singular boob (uniboob or symmastia).
Repair: Your surgeon will remove any scar tissue that is present, then extend the breast pockets—both laterally and superiorly—to allow space for the implants to be repositioned away from the middle of your chest. In doing this, your surgeon creates better separation between the two breasts. He will also reattach the fat and underlying breast tissue to the breastbone using permanent sutures to hold the sternal skin down. Additional sutures are used to reinforce the breast pocket so that it is closed and provides a barrier that prevents the implants from merging toward each other.
4. High-riding implants (high malposition)
After breast augmentation, every woman waits in anticipation for the moment their breasts drop and fluff. But for some, it never happens. The implants ride high—giving fullness up top and nothing below—while the nipples turn downwards. This may be the result of the breast pocket being created too high on the chest, fluid filling the implant pocket, muscle fibers tensing up in the lower pole of the breasts, or scar tissue developing around the implant (capsular contracture). In other cases, the implants settle higher in the pocket during the healing process and simply fail to drop.
Repair: The type of breast revision surgery will depend on what's causing the implants to sit high. That said, of all the types of implant malposition, this is perhaps the easiest to correct through releasing the breast tissue, removing scar tissue, and downsizing the implant size.
5. Lateral implant displacement
When the pocket spaces for the implants are made too large or are spaced too far to the sides, the implants can spill into the armpits, especially upon lying down. The breasts may appear too far apart from each other and the nipples shift inward, pointing toward the middle of the chest. This can happen if your breastbone sticks too far out, your tissues weaken under the weight of the implants, or your pectoralis muscle (in the case of under the muscle placement) contracts and force the implants to move outward.
Repair: Lateral implant displacement can be corrected by reinforcing the pocket with mesh, acellular dermal matrix or permanent sutures, or by creating a new pocket either above or below the pectoral muscle.
Breast deformity and natural occurrences of the breasts
Some women have congenital breast deformities or their breasts change over time due to gravity, aging, weight loss, pregnancy or other factors. It causes the breasts or nipple-areola complex to be abnormal in appearance. Not choosing to correct these problems before or during breast augmentation can make them worse, leading to breast revision surgery later.
6. Snoopy deformity
the prominence of the nipple-areolar complex is characterized by herniation of some of the breast tissue into the nipple-areolar complex. This may be due to the woman's own breasts or a result of having augmented breasts with heavy ptosis (breast sag).
7. Tuberous breasts: characterized by a narrow base of the breast, this occurs when a widening of the breast near the nipple-areolar complex happens, and a short or deficient inframammary crease manifests.
8. Mondor's cord (aka Mondor's disease): a thrombophlebitis of the superficial vein(s) of the breast. It is typically pronounced between the nipple and the inframammary crease and can cause significant discomfort. It is usually treated with anti-inflammatory medications and warm compresses until spontaneous resolution occurs.
9. Thinning of the breast tissue: a result of aging, pregnancy or breastfeeding, the implants become more visible and the appearance less natural.
10. Sagging breasts: Over time as tissue elasticity is lost, the skin becomes elongated and the breasts sag. This is most commonly the result of aging, sun damage, smoking or having large, weighty breasts.
Implant malfunction or dissatisfaction
Implants aren't perfect devices; sometimes they malfunction. Other times, it's not the implant itself, rather it's the patient's dissatisfaction with size or the patient's own body rejecting the implant and putting some of its functions into overdrive.
- Deflation (implant rupture): this issue is usually obvious because the saline implants’ augmentation effect is rapidly lost in the course of a day or two. Although the saline solution is harmlessly absorbed by the body, replacement of the implant should be performed within a few weeks to keep the pocket from shrinking. With silicone implants, any ruptures may be less obvious and may require further testing to confirm, such as an ultrasound or MRI exams. Most implants used today have a full replacement warranty that will provide you with replacement implant(s) at no cost to you.
- Capsular contracture: when your body forms a thick scar around the implant(s), it is known as capsular contracture. This may occur on one or both sides and may cause a shape change, discomfort, and may cause the breast to feel firm. It may be more common following infection or hematoma. Capsular contracture is less common and less severe with saline implants than with silicone implants.
- Dissatisfaction with implant size: either too small or too large, this is the most common reason why women have a second operation to change the size of their implants and more commonly select a larger implant. Dissatisfaction with your implant size is typically preventable by using a thorough evaluation and decision-making process.
Combination problems
There are times when the patient's body, implant, and surgical technique all work together to create a problem.
- Double-bubble: this is an issue where there is the appearance of the round breast sitting on top of a round breast implant. This may represent a problem with the tissue characteristics as well as a problem with the surgical placement of the implants and may occur on one or both sides.
- Rippling and implant palpability: this happens when irregularities of the implant surface are felt or seen through the skin. This may develop as a result of a thinning of the tissue covering the implants, caused by an implant that is either under-filled or leaking.
Breast revision surgery: solutions to breast augmentation complications
No matter what the problem or concern with your initial breast augmentation may be, a specific solution exists. Here are the most common corrective procedures for the issues list above. Remember to consult your doctor before pursuing a corrective procedure.
- Implant exchange: this is a procedure where a surgeon replaces your present implants with new ones that may be smaller or larger, overfilling to change the appearance of the implants in an effort to reduce rippling. He/she will likely change the present shape of your implants to a new shape such as high profile, smooth or anatomical implants. This changes the surface of the implants from smooth to textured or vice versa, or changes the filling of your implants from saline to silicone or vice versa.
- Capsulectomy: involves removing the entire capsule surrounding the implant. This is the definitive, state-of-the-art treatment for capsular contracture and may be combined with moving the implants into a totally submuscular position, and even an exchange to a textured surface implant may be performed to reduce recurrence rates.
- Capsulotomy: involves making incisions in the capsule surrounding the implants to open the space and make more room for them. In the opinion of some surgeons, this is an unsatisfactory solution for capsular contracture but is very useful to reposition implants.
- Placement change: where a surgeon moves the implants from above the muscle to below the muscle, or vice versa.
- Mastopexy (breast lift surgery): an operation used to remove excess skin and breast tissue, then pull them together with sutures to provide lifted and more shapely breasts.
- Internal pocket adjustment: used for implants that have bottomed out or for other position problems, the pocket is readjusted and positioned in the center, behind the nipple.
- Symmastia repair: this involves reattaching the fat and underlying breast tissue to the breastbone. If there is any scar tissue, it is removed. Sutures are set in place to hold the sternal skin down and to keep the pocket closed.
- Areolar reduction: tiny incisions are made around the outer border of the areola, then excess tissue and areolar skin are trimmed.
- Correction of a "Snoopy" deformity: entails using an incision around the outer border of the areola, then lifting the breast tissue higher on the chest, along with the nipple-areola complex. This allows the nipple-areola complex and breast mound to sit directly above the implants.
- Correction of a tuberous breast deformity: the tissue in the lower breast pole is released, allowing the base of the breast to expand. If the constriction is enough, either an inflatable implant or tissue expander is inserted. This helps stretch the tissue under the breasts. It may also include lifting the nipples higher on the chest mound or performing a breast lift to raise the position of the breasts and areolas and to give the breasts a more shapely appearance.
- Correction of natural asymmetry: may require implants of different sizes or shapes as well as adjustment of the inframammary crease on one or both sides.
Breast implant revision photos
Double bubble/Capsular contracture
/Bottoming out/Implant asymmetry repair
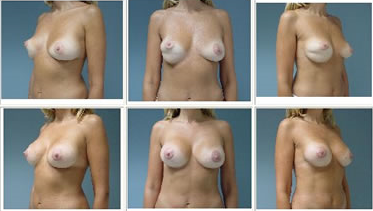
Procedure: Left Breast Capsulectomy,
"Internal Bra" with Implant Exchange
Age: 45, 5'7", Weight: 130, 34B to 34C, Smooth, Round Saline Implants filled to 200cc replaced with Mentor Smooth, Round Saline Implants filled to 325cc, Incision: Periareolar, Placement: Subpectoral, 3 Months Post-op
(Note: Dr. Don Revis performed the revision, not the initial procedure)
Want to find out if you need breast revision surgery?
Do you have any of the problems we discussed? If so, reach out to our network of plastic surgeons to find out what your specific treatment options are. Ultimately it will come down to your treating surgeon, but at least you'll have an idea when you walk in what your corrective procedure might consist of.
